Zhen-Hong Pan,
Yan-Xuan Zhang ![]() ,
Jun Fang,
Qing-Shan Qu,
Xin Jiang,
Ming Li
,
Jun Fang,
Qing-Shan Qu,
Xin Jiang,
Ming Li
For correspondence:- Yan-Xuan Zhang Email: zyxzhangpjms@163.com
Received: 7 October 2015 Accepted: 7 April 2016 Published: 27 May 2016
Citation: Pan Z, Zhang Y, Fang J, Qu Q, Jiang X, Li M. Clinical effects of sirolimus treatment in patients with increased serum creatinine levels after renal transplant. Trop J Pharm Res 2016; 15(5):1077-1081 doi: 10.4314/tjpr.v15i5.25
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To observe the clinical effects of sirolimus (SRL) immunosuppressive therapy in patients with progressively increasing levels of serum creatinine (Scr) after renal transplant.
Methods: In total, 180 patients whose Scr levels had been rising after renal transplant were given an oral calcineurin inhibitor (CNI): either cyclosporine A (CsA) or tacrolimus (FK506). All patients were treated at People’s Hospital of Zhengzhou, China, between January 2011 and December 2013, and were given SRL-based conversion treatment. Scr level and glomerular filtration rate (GFR) were observed before and 1, 3, and 6 months after treatment initiation. In addition, liver function, blood glucose, blood lipid levels, rejection reaction incidence, and mortality were recorded to evaluate the effects of SRL.
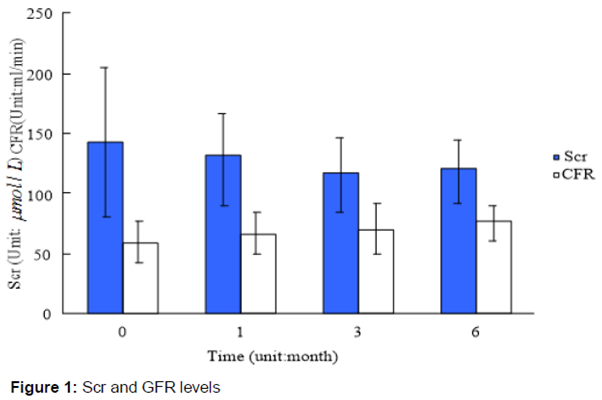
Results: Scr levels were 116.60 ± 30.60 μmol/L and 119.00 ± 24.60 μmol/L, and GFR was 70.00 ± 19.70 mL/min and 75.90 ± 15.60 mL/min, at 3 and 6 months after treatment, respectively. The 3- and 6-month Scr and GFR values were statistically different (p < 0.05) compared to pre-treatment levels (Scr: 144.10 ± 61.70 μmol/L vs and GFR: 59.10 ± 16.20 mL/min. Acute rejection (AR) occurred in 20 patients (13.30 %) within 6 months of treatment initiation, but rejection was reversed with conventional methylprednisolone therapy. Twenty-one patients (11.70 %) developed lung infections, but all were cured. There were no significant differences in liver function before and after treatment.
Conclusion: SRL-based immunosuppressive therapy is effective in treating patients with increased Scr levels after renal transplant.
Introduction
The extensive application of novel immunosuppressors has led to a dramatic reduction in acute rejection (AR) incidence; however, long-term survival after renal transplant is still not adequate [1,2]. The key factors influencing patient and kidney survival include liver and kidney toxicity, diabetes occurrence, chronic allograft nephropathy, and malignant tumors occurring after transplant [3,4]. Calcineurin inhibitors (CNIs) are currently the most commonly used immunosuppressors in renal transplant patients, and CNI treatment significantly improves survival rates after transplantation. However, chronic allograft nephropathy (CAN) is caused by renal toxicity, which can be induced by CNI treatment. The occurrence of CAN due to immunosupressor treatment has increased research interest in the transplantation field [5].
Serum creatinine (Scr) levels progressively increase after transplantation in kidneys that enter the decompensation period after CAN. If this decompensation fails to be controlled, transplanted kidney function will be lost. However, the development of new immunosuppressors, such as sirolimus (SRL), make it possible to stop CNI treatment [6]. Treating renal transplant patients with immunosuppressive drugs other than CNIs has received more attention in recent years. SRL, a new generation of powerful immunosuppressor, has less renal toxicity as well as anti-proliferative and anti-tumor effect [7]. SRL treatment represents a potential alternative to CNIs for renal transplant patients. Therefore, the prevention of complications and improvement of long-term survival rates in renal transplant patients has attracted a lot of attention in recent years. Currently, researchers are trying to find an alternative but equally effective treatment to CNIs. In this study, 180 patients who developed CAN after renal transplant at Zhengzhou People’s Hospital between February 2011 and December 2013 were treated with SRL conversion therapy.
Methods
Subjects
In total, 180 patients who developed CAN after renal transplant were selected from Zhengzhou People’s Hospital between February 2011 and December 2013. Of the 180 cases, 120 were male and 60 were female, with ages ranging from 27 to 49 years (mean, 38.60 ± 2.40 years). Conversion treatment started, on average, (46 ± 10) months after transplantation. Before conversion treatment, 103 cases were given cyclosporine A (CsA) + mycophenolate mofetil (MMF) + prednisone-combined immunosuppressive therapy while 77 cases were given tacrolimus (FK506) + MMF + prednisone-combined immunosuppressive therapy. All patients gave written informed consent; the study has been approved by People’s Hospital of Zhengzhou Ethics Committee (approval no. QGYZ201503901) and it followed the guidelines stipulated by the Ethics Committee [8].
Selection criteria
Patients with the following traits were selected: stable transplant kidney function with Scr level >140 μmol/L and increased blood pressure and proteinuria 6 months after kidney transplant; patients with CNI-induced hepatotoxicity or abnormal liver function after transplant; patients with diabetes or hyperglycemia after transplant that was controlled with hypoglycemic drugs or insulin; patients who had fibrosis in the transplant kidney confirmed by aspiration biopsy; and patients who had renal tubule atrophy combined with intimal hyperplasia but without AR. Patients who could not undergo immunosuppressive therapy due to a specific disease or financial conditions or who had serum cholesterol over 6 mmol/L, triacylglycerol over 2 mmol/L, 24-hour proteinuria over 0.80 g, peripheral blood leucocyte counts less than 3.5 × 109/L, and blood platelet counts less than 80 x 109/L were excluded.
Therapeutic schedule
SRL treatment began upon cessation of CNI treatment. Patients were given 3 - 6 mg/d SRL on the first day, and then 1 - 2 mg/d for 5 - 7 days. After 7 days, blood SRL concentration was maintained at 5 - 15 ng/mL by taking SRL orally. SRL concentration was controlled within the therapeutic window range. The dosage of other immunosuppressors remained the same.
Observation indices
Scr level and glomerular filtration rate (GFR) were detected before, and 1, 3, and 6 months after treatment initiation. AR incidence, infection rate, renal allograft dysfunction rate, and death rate were observed for 6 months after treatment. Liver function, blood glucose, blood parameters, and 24-hour proteinuria were measured before and after treatment initiation to detect adverse reactions.
Statistical analysis
SPSS 19.0 software was used to analyze the data. All values are expressed as mean ± standard deviation (SD). Comparison of means was performed using a non-paired t-test. Differences were considered statistically significant at p < 0.05.
Results
Analysis of AR and infection after conversion treatment
Of the 180 cases, 24 (13.30 %) experienced mild AR (level IA - IB) within 6 months of SRL treatment initiation, but all cases were successfully treated with cortical hormones. After AR treatment, all patients had stable renal function and no repeat AR. Of the 24 AR cases, 12 had no more AR incidents 6 months after cessation of cortical hormone treatment. No deaths or cases of kidney dysfunction were observed in the 6 months after SRL treatment initiation. Twenty-one patients (11.70 %) developed lung infections, including 12 cases of cytomegalovirus (CMV) infection (accounting for 57.10 % among infection cases), 6 cases of bacterial infection (28.60 %), and 3 cases of fungal infection (14.30 %); however, all patients were cured by traditional anti-infection treatments.
Changes in Scr and GFR before and after conversion treatment
Scr levels decreased and GFR increased in the first 6 months of treatment, with significant differences beginning in the 3rd month (p < 0.05) ().
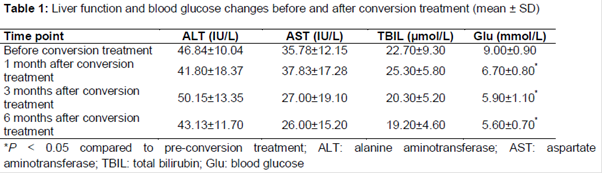
Changes in liver function and blood glucose
There were no differences in liver function before and after treatment (p > 0.05). Blood glucose levels were normalized after treatment, and this difference was significant (p < 0.05) ().
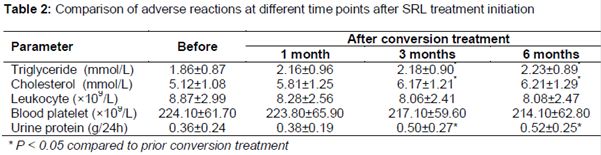
Adverse reactions
Of the 180 cases, 75 cases (41.70 %) had increased blood lipid levels after SRL treatment, with 24 cases of increased triglyceride (accounting for 32 % among all cases with increase blood lipids), and 51 cases of increased cholesterol (68 %); In addition, 9 patients (5 %) had decreased leukocyte counts, 6 had (3.30 %) decreased platelet counts, and 60 (33.30 %) had increased urine protein. Except for blood platelet and leukocyte counts, the other measures described here were significantly different 3 and 6 months after treatment initiation (p < 0.05) ().
Discussion
Immunosuppressors are an indispensable tool for organ transplantation success. Individual differences and an insufficient understanding of the immune system can affect the development of effective immunosuppressive drugs [9].
CNI treatment is known to have a stable and anti-rejection effect on transplant patients; however, renal toxicity induced by long-term CNI treatment is a significant issue and occurs in the majority of CNI-treated patients. Nankivell et al [10] found that 68 % of patients with CNI-induced renal toxicity had CAN 1 year after transplant; 62 % of patients treated with FK506 developed CAN 2 years after transplant; and 72 % of patients treated with CsA developed CAN 2 years after transplant. Therefore, reducing or avoiding CNI treatment can lower the incidence of CAN and improve long-term survival rates in transplant patients, as well as increasing transplant organ survival.
SRL, a new generation of immunosuppressor, is characterized by reduced renal toxicity. SRL is mainly metabolized in the liver and gastrointestinal tract through the cytochrome P450 system, and over 91 % of the metabolite product is expelled through the gastrointestinal tract, and a further 2 % is expelled through the skin [11,12]. SRL prevents the transition from G1 phase to S phase in T lymphocytes, and can therefore prevent interleukin-2 (IL-2) receptor binding and Tc and Td cell sensitization [13]. In addition, previous studies have shown that SRL also has anti-proliferative and anti-tumor effects [14,15] SRL can be an alternative treatment to CNI for patients who develop tumors or CAN after rental transplant.. In this study, Scr levels decreased and GFR increased in the 6 month period after SRL treatment initiation. Overall, SRL was effective at treating CAN.
Risk is inevitable when using a new immunosuppressor for conversion treatment. First, the occurrence of AR and excessive immunosuppression should be noted during treatment [16,17]. In this study, 24 cases experienced AR within 6 months of SRL treatment initiation, and this appeared to correlate with the withdrawal of FK506, unstable blood SRL concentration, absorption differences, and liver metabolism [18]. Lung infections usually occur when immunosuppression is excessive. Of the 180 cases, 21 developed lung infections within 6 months of conversion treatment initiation; however, all recovered after traditional anti-infection treatment and SRL dosage adjustment. This indicates that insufficient and excessive immunosuppression can be avoided during conversion treatment with SRL.
In addition, there were no remarkable differences in liver function after conversion therapy initiation, and blood glucose levels were normalized, suggesting that SRL had little influence on blood glucose levels. Adverse reactions included hyperlipidemia, proteinuria, and myelosuppression. In this study, 75 of 180 cases (41.70 %) had increased blood lipid levels after conversion treatment, with significant differences beginning 3 months after treatment initiation.
The increased lipid levels were found to be dose-dependent; therefore, blood lipid levels could be managed by decreasing the dose of SRL. Forty patients (33.30 %) experienced increased proteinuria, with significant differences beginning 3 months after treatment initiation. Although all patients continued SRL treatment despite proteinuria and its unknown mechanism of action, this may be a concern for the future potential treatment with SRL.
Conclusion
The findings show that renal function improved after conversion treatment, indicating that SRL was more effective than FK506. SRL-based immunosuppressive therapy is effective and safe for treating FK506-induced Scr increases; however, the optimal dose and treatment plan for SRL is yet to be determined.
Declarations
Acknowledgement
References
Archives


News Updates